Relational Health as Buffer to Trauma
One major learning for me in my NMT journey was Bruce Perry’s focus on relational health and how it can buffer traumatic experiences.
Often, when thinking about traumatic experiences, a lot of the focus is done on the event, the factors precipitating the event, the symptoms after the event, and there is a lot of talk about recovery and resilience.
What Bruce Perry talks about is the power of relational health. Some of his research based on NMT accumulation of data suggests that relational health can be a buffer to traumatic experiences. So much so, that Bruce Perry says that it is not the trauma that will predict someone’s trajectory of recovery, but their current relational health.
When thinking about brain development, it is also the timing of the trauma that will have a critical impact. For instance, when repeated relational trauma happens early on in development, it may be harder for individuals to recover from it than when it happens later on during childhood. But again, one of the major factors of recovery according to Bruce Perry is the current relational health.
By relational health, Bruce Perry means support network: the quality and quantity of supportive relationships one has around them.
I cannot find a video on this at this time, but the Psychotherapy Networker has a free article (after you create an account) about a conversation between Bruce Perry and Gabor Maté about ACEs (Adverse Childhood Experiences) (see link here) and here is what Bruce says:
”You can have a horrific history, but if in the present moment you’ve got good relationships, are connected to your culture, and feel like you belong to a community, you have a tremendous therapeutic buffering. With that buffering, healing opportunities take place.
Similarly, with people who are struggling, how connected they were to family, community, and culture on their pathway to the present is a better predictor of their struggles than their ACE score. If you had some of those connections, while you might have absorbed some toxicity in your early life, you also had tremendous opportunities to counteract the effects.”
Another major point about ACEs that may be misunderstood is that the research is valid at a population level, not at an individual level. This is a very important part to understand when reading or hearing about research findings and how they apply clinically, but this may be for another blog article.
What does this mean clinically?
Clinically, I personally find it very hopeful. It also makes me focus beyond the individual and looking at support network. Similarly to what one may think about when we think about supporting people with neurodivergence, for developmental trauma (i.e. repeated relational-attachment trauma and shock trauma) we want to think about changing and adapting the environment to the need of the individual to set them up for success.
Bruce Perry has this NMT concept of the Therapeutic Web, where each interaction with an individual is creating these opportunities for healing.
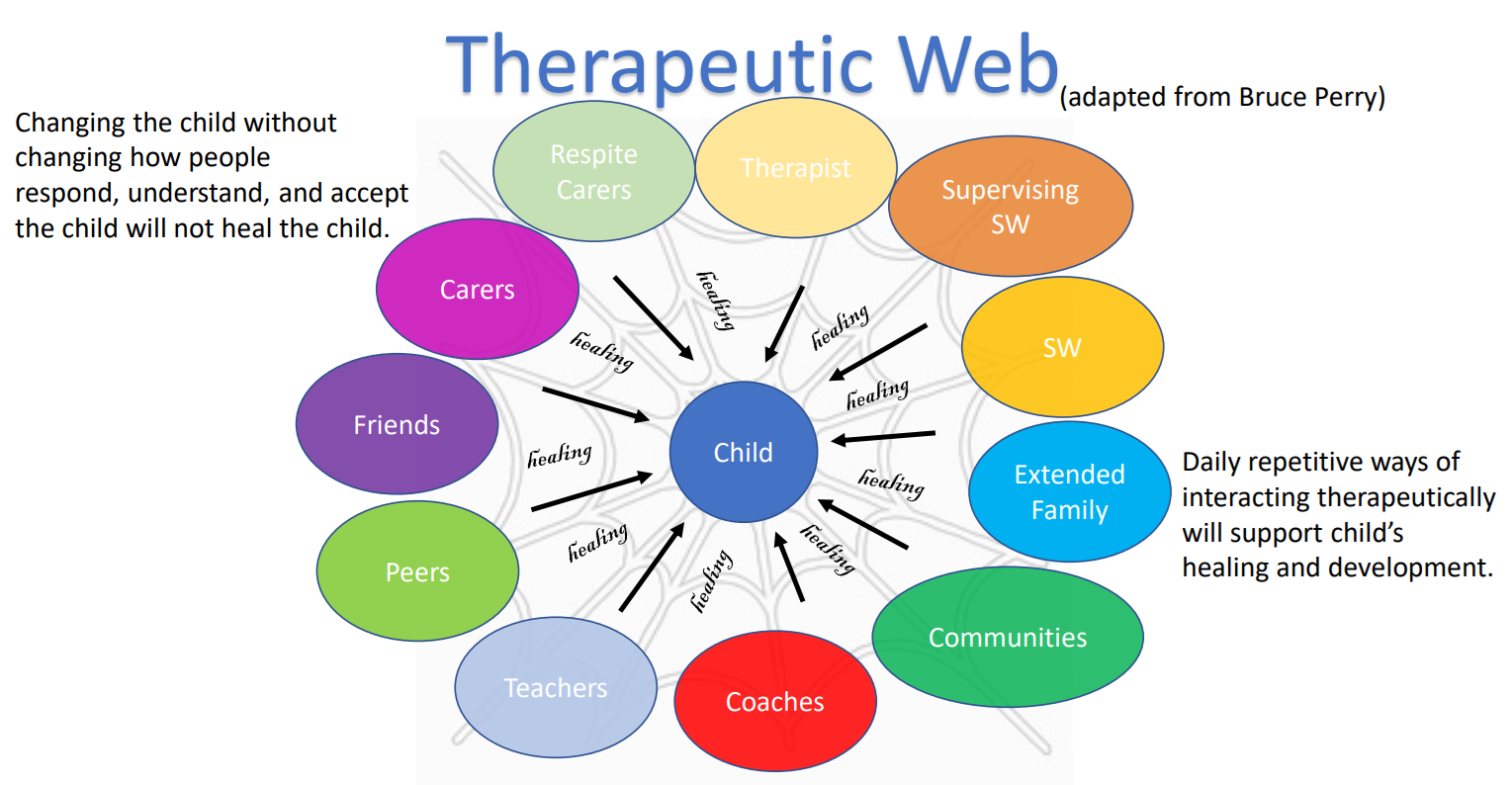
Therapeutic Web around a child. Child is at the centre interacting with adults and peers around them where daily repetitive positive interactions can create opportunities for healing.